Understanding Medicare Preventive Visits: Key Differences Between IPPE and AWV Services
Discover how understanding these distinctions can enhance patient care and ensure compliance.
Preventive care plays a crucial role in maintaining the health and well-being of Medicare beneficiaries. Two key services under Medicare's preventive care umbrella are the Initial Preventive Physical Examination (IPPE) and the Annual Wellness Visit (AWV). Although both enhance patient health, their purpose, eligibility, and components are distinct. We will aim to clarify these differences, helping healthcare providers optimize their delivery of these essential services.
What is the Initial Preventive Physical Examination (IPPE)?
The IPPE, commonly known as the Welcome to Medicare visit, is a one-time preventive exam available to new Medicare beneficiaries within the first 12 months of their Part B enrollment. The primary goal of the IPPE is to establish a baseline of the patient’s health and facilitate early detection of potential health issues.
Key Components of the IPPE
- Medical and Social History Review: Gathering comprehensive information on the patient's health and social background.
- Risk Factor Identification: Evaluating risks for depression, functional ability, and safety, as well as screening for potential substance use disorders (SUDs).
- Physical Exam: While not extensive, it includes a visual acuity screen and measurement of height, weight, BMI, and blood pressure.
- End-of-Life Planning: Offered if the patient desires, this component involves discussing advance directives and care preferences.
- Education and Counseling: Providing advice and referrals for preventive services.
The IPPE’s focus on early detection and prevention makes it a valuable tool in a patient’s initial encounter with Medicare services.
Understanding the Annual Wellness Visit (AWV)
The AWV is available to Medicare beneficiaries annually, beginning 12 months after their Part B coverage starts and after completing the IPPE. Unlike a traditional physical exam, the AWV is not a hands-on examination but a comprehensive review of a patient’s health status, emphasizing prevention and wellness.
Key Components of the AWV
- Health Risk Assessment (HRA): A questionnaire that evaluates the patient’s health risks and provides a foundation for the personalized prevention plan.
- Personalized Prevention Plan: A detailed plan based on the HRA, tailored to the patient’s needs, including a 5- to 10-year screening schedule.
- Cognitive Impairment Detection: Assessing the patient for any signs of cognitive decline.
- Medical and Family History Review: Updating the patient’s medical records to reflect current conditions and family health history.
- Education and Referrals: Offering personalized health advice and referrals for preventive services, including advance care planning if requested.
The AWV’s focus on prevention, risk assessment, and personalized health management sets it apart from other routine medical exams.
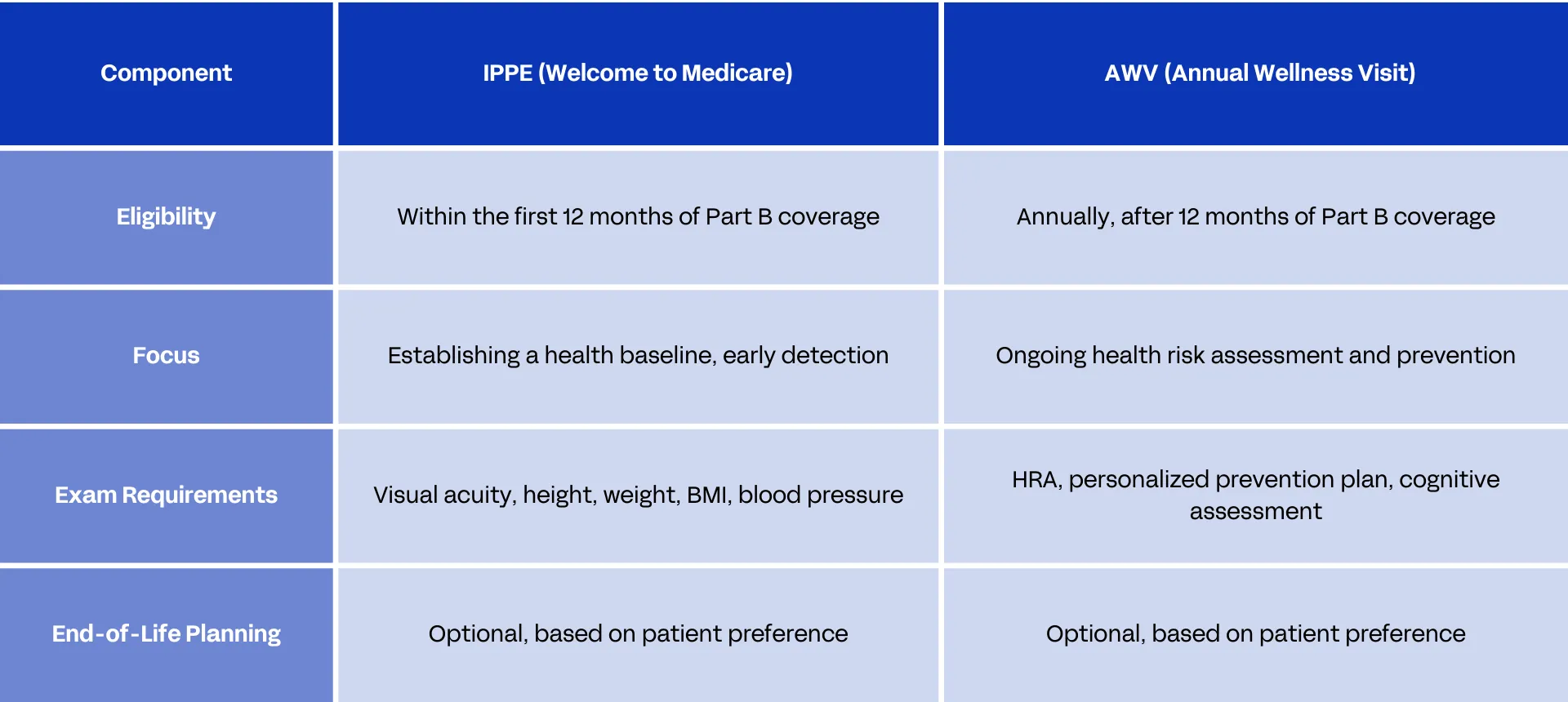
Comparing IPPE and AWV
While both the IPPE and AWV aim to promote health and prevent disease, they differ significantly in their approach:
Ensuring Compliance with Documentation and Coding
Accurate documentation ensures compliance and appropriate reimbursement for IPPE and AWV services. Common documentation pitfalls include incomplete health risk assessments, missing family history, and conflicting documentation regarding cognitive impairment. Providers should carefully document all components to avoid errors leading to denied claims or improper billing.
Quick Coding Guide
- IPPE: Use code G0402
- Initial AWV: Use code G0438
- Subsequent AWVs: Use code G0439
It's essential to report a diagnosis code that accurately reflects the patient's condition during these visits. For example, use Z00.00 for a general adult medical examination without abnormal findings and Z00.01 if there are abnormal findings.

Practical Tips for Providers
- Ensure Thorough Documentation: In IPPE and AWV documentation, avoid missing key components like family history or SUD screenings.
- Update Annually: Ensure the HRA and personalized prevention plan are updated annually during the AWV.
- Educate Patients: Clearly explain the differences between the IPPE and AWV to patients, helping them understand the benefits of each service.
Looking Ahead: The Future of Preventive Care in Medicare
As healthcare continues to evolve, so will the components and requirements of preventive services like IPPE and AWV. Future trends may include enhanced use of technology for risk assessment, policy changes affecting coverage, and a greater focus on personalized medicine. Staying informed about these changes will help healthcare providers continue to deliver high-quality, compliant care to Medicare beneficiaries.
We anticipate IPPE and AWV services will increasingly utilize a diverse care team, including pharmacists, Registered Nurses (RN), and dietitians. Organizations should look to optimize staffing, ancillary personnel involvement, and telehealth offerings as patient needs expand. Additionally, we anticipate increased scrutiny of preventive medicine documentation as witnessed in the 2024 $11.7 million Penn State settlement over false claims allegations relating to Medicare Annual Wellness Visits.
In conclusion, understanding the differences between the IPPE and AWV is crucial for healthcare providers. By ensuring proper documentation and staying informed on current and future guidelines, providers can maximize the benefits of these preventive services for their patients.
.webp)
